
When the Diabetes Lab Test Lies: The Hidden Impact of G6PD Deficiency on Diabetes Care
Why the same HbA1c result can reflect dramatically different levels of hyperglycemia and may contribute to delayed diagnosis, delayed treatment, and worse diabetes outcomes.

Black Americans are nearly twice as likely to develop kidney failure from diabetes and experience substantially higher rates of amputations, cardiovascular disease, and diabetes-related death.
Most explanations focus on socioeconomic factors and healthcare access.
But what if part of the problem lies in a laboratory test used millions of times every day?
What if many Black patients are being told their diabetes is less severe than it really is?
Have you ever wondered why your continuous glucose monitor seems much worse than your HbA1c? Approximately one in ten Black American men carries G6PD deficiency, one of the most common inherited enzyme deficiencies in the world.
Hemoglobin A1c (HbA1c) testing has become the central test used by doctors to diagnose and manage diabetes treatment. HbA1c measures the percentage of hemoglobin molecules inside red blood cells that become coated with glucose over time. Since red blood cells normally circulate in the bloodstream for approximately three months, HbA1c provides physicians with an estimate of the average blood glucose level over the preceding weeks.
Doctors use HbA1c constantly:
to diagnose diabetes,
to estimate disease severity,
to decide whether treatment should be intensified,
to monitor long-term glucose control,
and in many healthcare systems, to determine eligibility for advanced medications.
But HbA1c depends on something many people do not realize:
the lifespan of red blood cells. This means that two patients may have exactly the same HbA1c result, look identical on paper, but biologically, they may be experiencing very different diabetes.
If red blood cells break down earlier than usual, they have less time to accumulate glucose. HbA1c values may then appear artificially low, even when glucose levels are dangerously elevated.
One of the most common conditions affecting red blood cell survival is Glucose-6-Phosphate Dehydrogenase (G6PD) deficiency.
G6PD deficiency is the most common enzymatic deficiency in humans, affecting more than 400 million people worldwide. It is particularly common among individuals of African, Mediterranean, Middle Eastern, and parts of Asian ancestry. In the United States alone, approximately 10% to 14% of Black American men carry G6PD deficiency.
Yet despite its enormous prevalence, G6PD deficiency remains largely overlooked in diabetes care.
In our recent studies using nationwide longitudinal electronic health records from Israel, we examined more than two decades of data comparing thousands of individuals with G6PD deficiency to matched controls.
The findings were striking.
At the same glucose levels, HbA1c values were substantially lower in patients with G6PD deficiency. A HbA1c value of 6.5%, the standard diagnostic threshold for diabetes, corresponded to fasting glucose levels around 168 mg/dL in men with G6PD deficiency, compared with 126 mg/dL in the general population.
This means that many patients with significant hyperglycemia may appear substantially less diabetic than they truly are.
The scatter plots below illustrate this phenomenon.
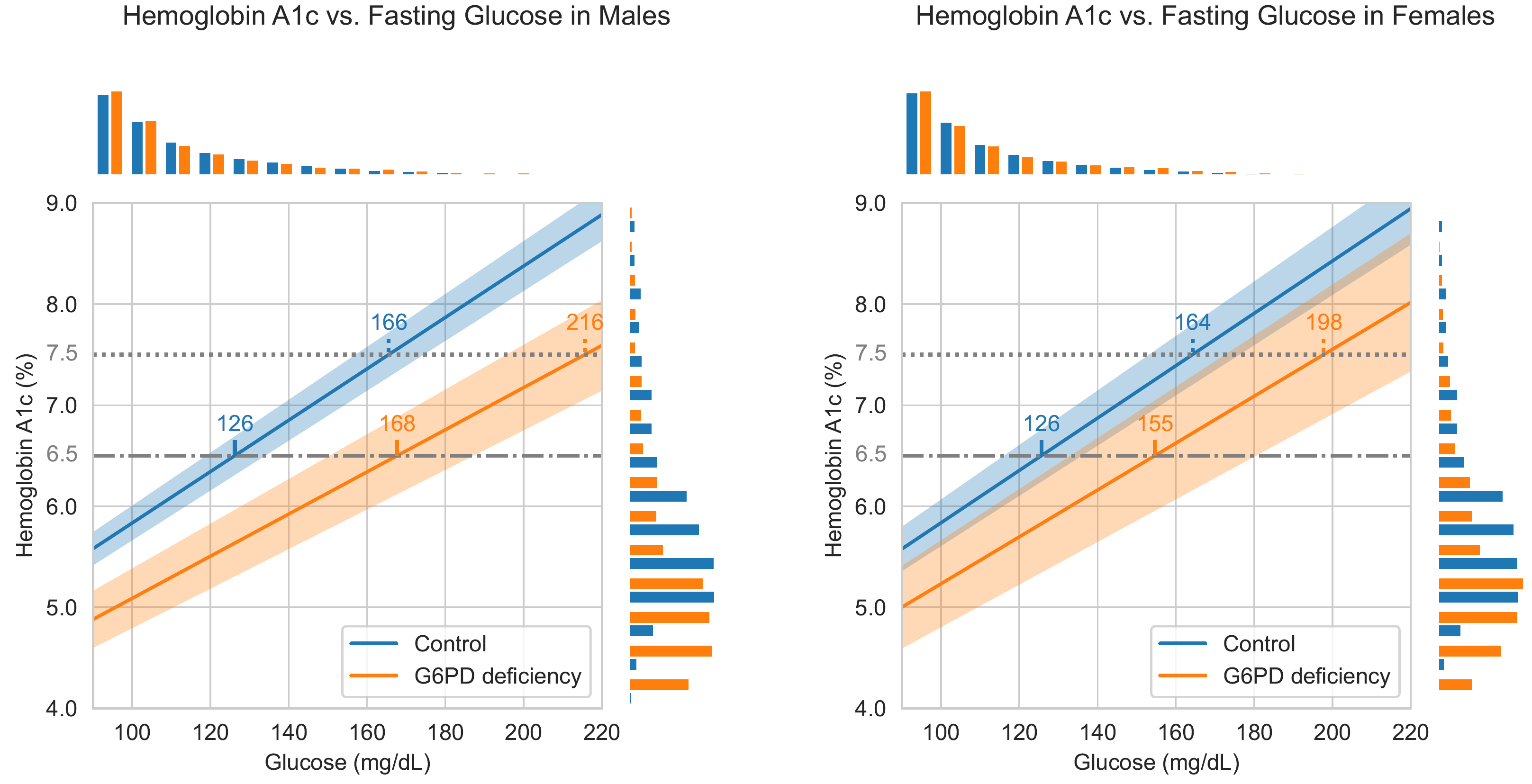
Each point represents paired glucose and HbA1c measurements obtained from individual patients. The blue regression line represents individuals without G6PD deficiency, while the orange line represents individuals with G6PD deficiency. At every glucose level, HbA1c values in G6PD-deficient individuals are shifted downward.
The consequences are not subtle. In men with G6PD deficiency, the standard diagnostic HbA1c threshold of 6.5% corresponded to fasting glucose levels of approximately 168 mg/dL, compared with 126 mg/dL in the general population.
Moreover, the discrepancy becomes even larger as glucose levels rise. Patients with G6PD deficiency may appear well controlled on paper while experiencing a substantially higher glycemic burden in reality.
For example, an HbA1c value of 7.5%, which is often considered reasonably acceptable in some patients, corresponds to glucose levels of approximately 165 mg/dL in the general population. In contrast, among men with G6PD deficiency, the same HbA1c value corresponds to glucose levels exceeding 210 mg/dL.
In practical terms, an HbA1c value of 7.5% in a man with G6PD deficiency reflects a degree of hyperglycemia that, in the general population, would typically be associated with HbA1c values approaching 9%.
In other words, two patients may carry exactly the same HbA1c value while having dramatically different degrees of hyperglycemia.
The larger effect observed in men is not incidental.
The G6PD enzyme is encoded on the X chromosome. Because males carry only one X chromosome, a defective G6PD gene usually affects nearly all of their red blood cells, often producing more pronounced biological effects.
Females, however, carry two X chromosomes. Early during embryonic development, each stem cell randomly “switches off” one of the two X chromosomes. As a result, many women become biological mosaics: some of their red blood cells express the normal G6PD gene, while others express the deficient version. This partial “rescue” often reduces the severity of the condition in females, although the degree of protection can vary substantially between individuals depending on the proportion of cells expressing each X chromosome.
This has enormous clinical implications.
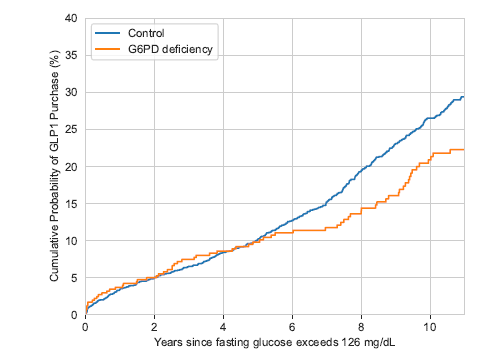
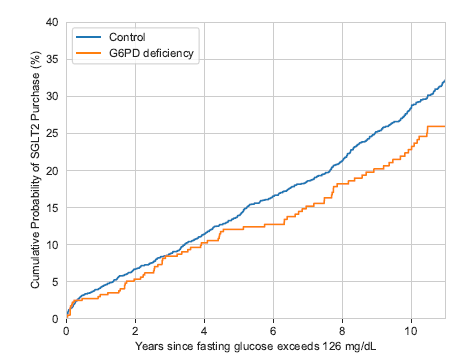
Modern diabetes care increasingly relies on powerful medications such as GLP-1 receptor agonists and SGLT2 inhibitors. These medications not only lower glucose, but also reduce cardiovascular disease, kidney failure, hospitalization, and mortality.
However, in many healthcare systems, access to these medications depends heavily on HbA1c thresholds.
If HbA1c systematically underestimates disease severity, patients may be diagnosed later, treatment may be intensified later, and access to newer therapies may be delayed despite objectively elevated glucose levels.
That is exactly what we observed.
To study this, we used a statistical approach called survival analysis.
Despite its name, survival analysis is not limited to mortality studies. It is a method used to analyze how long it takes until a particular event occurs. In our case, the “event” was not death, but the initiation of diabetes treatment or the development of severe diabetic complications.
The Kaplan-Meier curves below show the cumulative probability over time of patients receiving diabetes medications after meeting objective criteria for diabetes based on glucose levels.
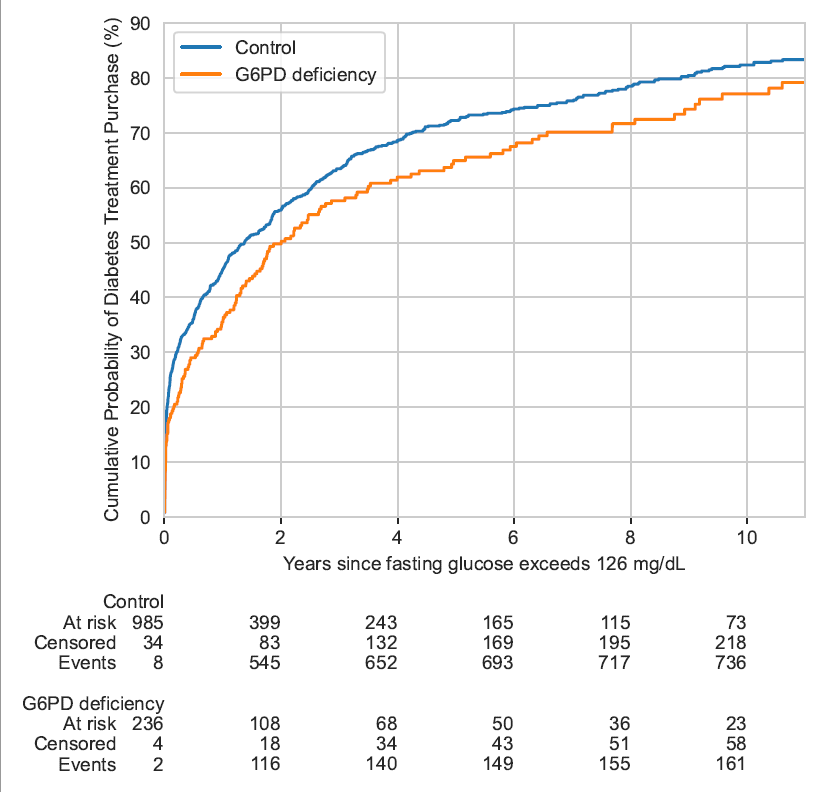
The curves clearly demonstrate that patients with G6PD deficiency experienced substantial delays in treatment initiation after their fasting blood test first reached daiebetes levels.
The problem extends beyond individual clinical decisions. Many treatment guidelines and reimbursement policies use HbA1c thresholds to determine eligibility for advanced therapies. When HbA1c systematically underestimates disease severity, structural inequities can emerge even when clinicians follow existing guidelines correctly.
Patients with G6PD deficiency were significantly less likely to receive the newer classes of diabetes medications - particularly GLP-1 receptor agonists (such as Victoza, Trulicity, and Ozempic) and SGLT2 inhibitors (such as Jardiance and Forxiga) - therapies that have revolutionized our ability to reduce diabetes complications, kidney failure, cardiovascular disease, and mortality.
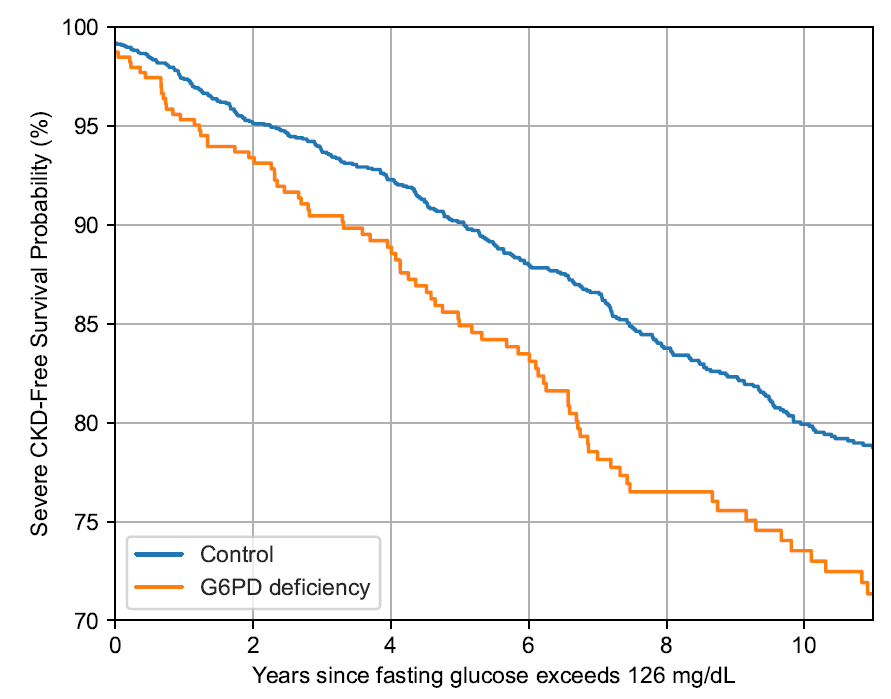
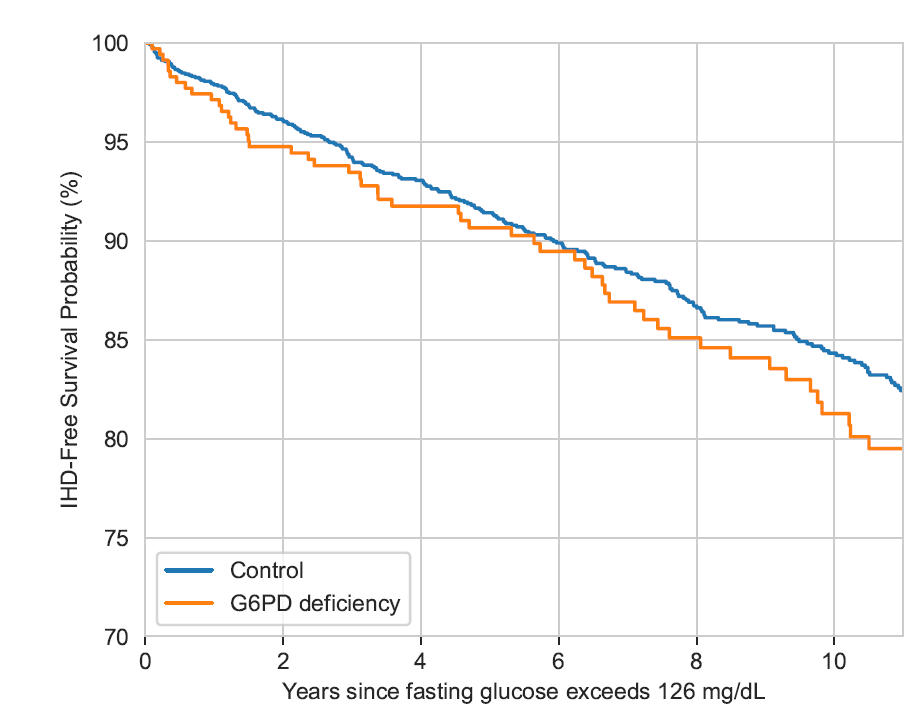
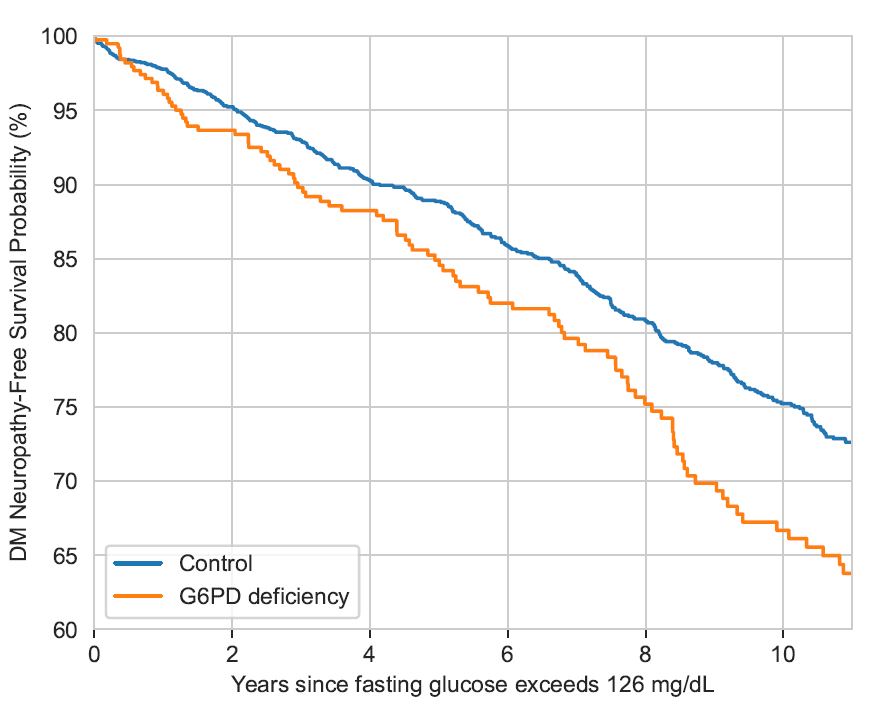
At the same time, these patients experienced markedly higher rates of severe diabetic complications, including kidney disease, cardiovascular complications (myocardial infarction, stroke), and diabetic neuropathy.
Paradoxically, reliance on HbA1c may not only contribute to undertreatment, but potentially worsen the biological dynamics of diabetes itself.
Some older diabetes medications, particularly sulfonylureas, may increase oxidative stress within red blood cells. In patients with G6PD deficiency, whose red blood cells are already vulnerable to oxidative damage, this may accelerate hemolysis - the breakdown of red blood cells.
As red blood cells are destroyed more rapidly, HbA1c values may fall even further, creating the illusion of improving diabetes control despite worsening hyperglycemia.
In other words:
the biomarker itself may become progressively misleading precisely in the patients who are at highest risk.
Importantly, this problem is not limited to one ethnic group or one country.
Similar effects of G6PD deficiency on HbA1c levels have now been reported in African-American populations and East Asian populations carrying distinct G6PD genetic variants.
This suggests that a substantial fraction of diabetes inequity observed worldwide may partly reflect hidden biological bias embedded within one of medicine’s most widely used laboratory tests.
The encouraging aspect is that this inequity may be remediable.
Awareness can change treatment decisions.
Clinicians caring for patients from high-prevalence populations should recognize that HbA1c may substantially underestimate glycemic burden in G6PD-deficient individuals. Alternative approaches, including fasting glucose measurements, continuous glucose monitoring, fructosamine, glycated albumin, or modified interpretation of HbA1c values, may improve care in these populations.
Large-scale health data sometimes reveals hidden biological patterns that remain invisible at the level of individual patients.
This is one of them.
For millions of people worldwide, HbA1c may not tell the whole story.
Recognizing when it fails could lead to earlier diagnosis, better treatment, and fewer diabetes complications.
References:
Type 2 Diabetes in Patients with G6PD Deficiency.
The New England journal of medicine. 2024 Aug 8; 391(6):568-569.
Israel A, Raz I, Vinker S, Magen E, Green I, Golan-Cohen A, Berkovitch M, Merzon E.
doi: 10.1056/NEJMc2406156.
More on Type 2 Diabetes in Patients with G6PD Deficiency. Reply.
The New England journal of medicine. 2024 Oct 31; 391(17):1664.
Israel A, Vinker S, Merzon E.
doi: 10.1056/NEJMc2411261#sa2.
Health disparities in diabetes treatment: The challenge of G6PD deficiency.
Diabetes research and clinical practice. 2025 Jan; 219:111965.
Israel A, Raz I, Green I, Golan-Cohen A, Berkovitch M, Magen E, Vinker S, Merzon E.
doi: 10.1016/j.diabres.2024.111965.